
Abstract
Objective
To evaluate the effects of a pulsating air bed on the relief of tissue oedema and duration of intensive care unit (ICU) stay of children post-cardiac surgery.
Design
Random allocation.
Setting
Paediatric cardiac ICU.
Patients and Participants
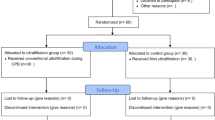
Sixteen patients, aged 3–48 months, who underwent the surgical repair of atrioventricular sepatal defect.
Intervention
The treatment group received continuous postoperative management on a pulsating low airloss bed. The control group was managed on a standard non-pulsating bed. The end point of the study was that total body water (TBW) returned to preoperative levels.
Measurements
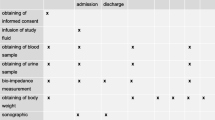
The TBW was measured by bioelectrical impedance and expressed as a percentage change of body weight as determined prior to treatment. Measurements were made before surgery, upon arrival on the ICU, and serially until TBW returned to preoperative levels. All patients were treated according to the standard ICU protocol, which includes strict fluid and diuretic regimens. Urine output, mean blood pressure and central venous pressure were measured.
Results
All patients developed a 2–20% increase in TBW above baseline after open heart surgery. Preoperative measurements and ICU admission values were identical. The maximum increase in TBW was reached 3–6 h after return to the ICU. These values were higher in the control group (p<0.01). The TBW returned to normal in the treatment group at 24 h after surgery, and at 48–72 h after surgery in the control group (p<0.001). There was a tendency for higher urine output and central venous pressure in the treated group. The duration of stay in the ICU was significantly less for the treated group (p<0.05).
Conclusions
Continuous air pulsation by a specialty ICU bed reduced TBW, relieved tissue oedema, and improved hemodynamics in oedematous post-operative paediatric cardiac surgery patients. This reduced morbidity may have cost-effective implications relating to decreased ICU stay and resource consumption. Further studies to evaluate the use of this technology in critically ill children are warranted.
Similar content being viewed by others

References
Maehara T, Novak I, Wyse RKH, Elliott MJ (1991) Perioperative monitoring of total body water by bio-electrical impedance in children undergoing open heart surgery. Eur J Cardiothorac Surg 5:258–262
Novak I, Davies PS, Elliott MJ (1992) Noninvasive estimation of total body water in critically ill children after cardiac operations.Validation of a bioelectric impedance method. J Thorac Cardiovasc Surg 104:585–589
Segal KR, Burastero S, Chun A, Coronel P, Pierson RN, Wang J (1991) Estimation of extracellular and total body water by multiple-frequency bioelectrical-impedance measurements. Am J Clin Nutr 54:26–29
Murai DT, Grant JW (1994) Continuous oscillation therapy improves the pulmonary outcome of intubated new-borns: results of a prospective, randomized, controlled trial. Crit Care Med 22:1147–1154
Elliott MJ, Hamilton JRL, Clark I (1990) Perfusion for Paediatric openheart surgery. Perfusion 5:1–8
El Habbal MH, Smith L, Strobel S, Elliott MJ (1993) Modified ultrafiltration after cardiopulmonary bypass for repair of ventricular septal defect reduces serum IL 8. Circulation 88:I-96
Stark J, de Leval M (1993) Surgery for congenital heart defects, Saunders, London
Author information
Authors and Affiliations
Additional information
This work was supported by a grant from Kinetic Concepts Incorporated, San Antonio, Texas, USA
Rights and permissions
About this article
Cite this article
Smith, L.J., El Habbal, M.H. Application of kinetics in intensive care management of children with generalized oedema. Intensive Care Med 22, 964–967 (1996). https://doi.org/10.1007/BF02044124
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02044124