
Abstract
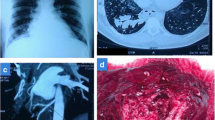
A bullectomy for spontaneous pneumothorax is often combined with pleurodesis to prevent recurrence. A recurrent or progressive residual bullous lung beneath adhesive pleura neovascularized from the chest wall may be affected by aspergillosis. Of the 12 patients with pulmonary aspergillosis secondary to bullous lung disease treated surgically at our hospital since 1974, 3 underwent a bullectomy with pleurodesis for spontaneous pneumothorax. The presenting symptoms in all cases were hemosputum. Aspergillus lesions affected the patients in the right upper lobe, the left apical segment, and both apical segments at 16, 9, and 13 years, respectively, after a bullectomy. Angiograms demonstrated hypervascularization in the intercostal and internal thoracic arteries, as well as in the bronchial branches. Catheter embolization for airway bleeding was not effective in 1 patient. Four operations, including an emergency procedure for massive intrapulmonary bleeding, were performed. These included a right upper lobectomy followed by a left upper segmentectomy at second-look operation in 1 patient who required bilateral chest wall resections. All patients survived the operations. Intraoperative bleeding ranged between 700 and 3500 ml (1543 ml on average), and bleeding foci were mainly from the chest wall, with hypervascularization stemming from the ipsilateral chest wall. Postoperative complications included pleural space hemorrhaging and a bronchopleural fistula, both of which required additional chest wall resections. Patients with bullous lung disease late after a bullectomy with pleurodesis may thus be associated with complex pleuropulmonary aspergillosis, which requires surgical therapy concomitant with a chest wall resection.
Similar content being viewed by others


References
Noppen M, Meysman M, d’ Haese J, Monsiear I, Verhaeghe W, Schlesser M, Vincken W (1997) Comparison of video-assisted thoracoscopic talcage for recurrent primary versus persistent secondary spontaneous pneumothorax. Eur Respir J 10:412–416
Trigt PV (1990) Lung infections and diffuse interstitial lung disease. In: Sabinston DC Jr, Spencer FC (eds) Surgery of the chest (5th edn). Saunders, Philadelphia, pp 634–638
Saraceno JL, Phelps DT, Ferro TJ, Futerfas R, Schwartz DB (1997) Choronic necrotizing pulmonary aspergillosis: approach to management. Chest 112:541–549
Glimp RA, Bayer AS (1983) Pulmonary aspergilloma: diagnostic and therapeutic considerations. Arch Intern Med 143:303–308
Purcell IF, Corris PA (1995) Use of nebulized liposomal amphotericin B in the treatment of Aspergillus fumigatus empyema. Thorax 50:1321–1323
Remy J, Amaud A, Fardou H, Giraud R, Voisin C (1977) Treatment of hemoptysis by embolization of bronchial arteries. Radiology 122:33–37
Roth C, Gebhart J, Just NG, von-Eisenhart RB, Beinhauer RI (1996) Characterization of amphotericin B aerosols for inhalation treatment of pulmonary aspergillosis. Infection 24:354–360
Hargis JL, Bone RC, Stewart J, Rector N, Hiller FC(1980) Intracavitary amphotericin B in the treatment of symptomatic pulmonary aspergillomas. Am J Med 68:389–394
Wex P, Utta E, Drozdz W (1993) Surgical treatment of pulmonary and pleuro-pulmonary Aspergillus disease. Thorac Cardiovasc Surg 41:64–70
Shirakusa T, Ueda H, Saito T, Matsuba K, Kouno J, Hirota N (1989) Surgical treatment of pulmonary aspergilloma and Aspergillus empyema. Ann Thorac Surg 48:779–782
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Endo, S., Sohara, Y., Murayama, F. et al. Late pleuropulmonary aspergillosis after the treatment of pneumothorax: Report of three cases. Surg Today 29, 1125–1128 (1999). https://doi.org/10.1007/s005950050658
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s005950050658