
Summary
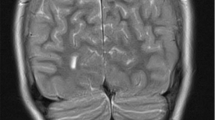
Autoimmune polyglandular syndrome is characterized by a failure of multiple endocrine organs and the presence of circulating organ-specific autoantibodies targeted against the failing organs. Here we describe a patient with autoimmune polyglandular syndrome type I with the endocrine manifestations of hypoparathyroidism, adrenocortical insufficiency, and insulin-dependent diabetes mellitus. Long-standing hypoparathyroidism led to extensive calcification of the basal ganglia which resulted in the clinical presentation of an extrapyramidal movement disorder (choreoathetotic and hemiballistic hyperkinesia of the left extremities). Interestingly, parallel to rehydration and the initiation of cortisol replacement therapy a complete reversion of the hyperkinetic signs was achieved. This case shows a rare multiendocrine organ failure with complex metabolic interactions resulting in marked neurological signs. Furthermore, this case demonstrates for the first time that a hyperkinetic syndrome - most likely due to hypoparathyroidism-induced basal ganglia calcification - can be reversed solely by adequate treatment of the concomitant endocrine failures.
Similar content being viewed by others


References
Ahohen P (1985) Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED): autosomal recessive inheritance. Clin Gen 27:535–542
Ahonen P, Myllärniemi S, Sipilä 1, Perheentupa J (1990) Clinical variation of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) in a series of 68 patients. N Engl J Med 322:1829–1836
Araki Y, Furukawa T, Tsuda K, Yamamoto T, Tsukaguchi 1 (1990) High field MR imaging of the brain in pseudohypoparathyroidism. Neuroradiology 32:325–327
Claude H, Gougerot H (1908) Insuffisance pluriglandulaire endocrinienne. J Physiol Pathol Gen 10:469–480
Eisenbarth GS, Jackson RA (1991)The immunoendocrinopathy syndromes. In: Wilson JD, Foster DW (eds) Williams textbook of endocrinology. Saunders, Philadelphia, pp 1555–1566
Friedmann JH, Chiucchini MAR, Tucci JR (1987) Idiopathic hypoparathyroidism with extensive brain calcification and persistent neurological dysfunction. Neurology 37:307–309
Hara T, Mizuno Y, Nagata M, Okabe Y, Taniguchi S, Harada M, Niho Y, Oshimi K, Ohga S, Yoshikai Y, Nomoto K, Yumura K, Kawa-Ha K, Ueda K (1990) Human γδ-T-cell receptor-positive cell-mediated inhibition of erythropoiesis in vitro in a patient with type I autoimmune polyglandular syndrome and pure red cell aplasia. Blood 75:941–950
Hoagland H (1954) Studies of brain metabolism and electrical activity in relation to adrenocortical physiology. Recent Prog Horm Res 10:29–63
Illum F, Dupont E (1985) Prevalence of CT-detected calcification in the basal ganglia in idiopathic hypoparathyroidism and pseudohyprathyroidism. Neuroradiology 27:32–37
Mann K(1989)Autoimmunerkrankungenendokriner Drüsen. Der Bayerische Internist 9:2–11
Muir A, Maclaren NK (1991) Autoimmune diseases of the adrenal glands, parathyroid glands, gonads and hypothalamic-pituitary axis. Endocrinol Metab Clin of North Am 20:619–645
Neufeld M, Maclaren N, Blizzard R (1980) Autoimmune polyglandular syndromes. Pediatr Ann 9:154–162
Neufeld M, Maclaren NK, Blizzard RM (1980) Two types of autoimmune Addison's disease associated with different polyglandular autoimmune (PGA) syndromes. Medicine 60:355–362
Orth DN, Kovacs WJ, DeBold R (1992) The adrenal cortex. In: Wilson JD, Foster DW (eds) Williams textbook of endocrinology. Saunders, Philadelphia, pp 578–619
Parfitt MA (1989) Surgical, idiopathic, and other varieties of parathyroid hormone-deficient hypoparathyroidism. In: DeGroot L (ed) Endocrinology, vol 2. Saunders, Philadelphia; pp 1049–1064
Roep BO, De Vries RRP (1992) T-lymphocytes and the pathogenesis of type 1 (insulin-dependent) diabetes mellitus. Eur J Clin Invest 22:67–711
Ropper AH, Martin JB (1991) Diseases of the spinal cord. In: Wilson JD, Braunwald E, Isselbacher K, Petersdorf RG, Martin JB, Fauci AS, Root RK (eds) Harrison's principles of internal medicine, 2th edn. McGraw Hill, New York, pp 2081–2088
Schmidt MB (1926) Eine biglanduläre Erkrankung (Nebenniere und Schilddrüse) bei Morbus Addisonii. Verh Dtsch Ges Pathol 21:212–221
Smits M; Gabreels F, Froeling P, Thijssen H, Colon E, ter Haar B, Ruland C, t'Lam R (1982) Autosomal dominant idiopathic hypoparathyroidism and nervous system dysfunction: report of three cases and review of the literature. J Neurol 228:113–122
Thomas L (1992) Labor and Diagnose. Medizinische Verlagsgesellschaft, Marburg
Van der Sande JJ, van Seters AP (1978) The adrenal gland: its relationship to neurology. In: Vinken PJ, Bruyn G (eds) Handbook of clinical neurology, vol 39. North-Holland, Amsterdam, pp 469–515
Author information
Authors and Affiliations
Additional information
Dedicated to Prof. Dr. G. Paumgartner on the occasion of his 60th birthday
Rights and permissions
About this article
Cite this article
Baumert, T., Kleber, G., Schwarz, J. et al. Reversible hyperkinesia in a patient with autoimmune polyglandular syndrome type I. Clin Investig 71, 924–927 (1993). https://doi.org/10.1007/BF00185605
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00185605