
Summary
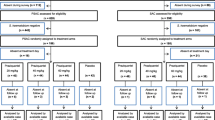
The degree of compliance during metrifonate therapy ofSchistosoma haematobium infection has been evaluated together with its impact on drug efficacy in two rural villages in Somalia. Drug treatment was offered to all subjects withS. haematobium infection. 243 subjects were screened for the presence of eggs in the urine using a sensitive Nucleopore filtration method and 211 were positive. All infected patients were put on a treatment schedule of 3 doses of metrifonate 7.5 mg/kg at fortnightly intervals. Drug efficacy was evaluated 6, 12 and 32 weeks after treatment.
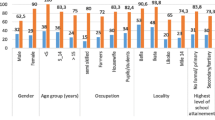
Only 48% of the patients took all 3 doses, 15% took 2 doses and 37% only took 1 dose. The cure rate was maximal in Week 6 at 60, 44 and 30% in those who took 3, 2 and 1 dose, respectively. Corresponding egg reduction rates were 98, 90 and 84%, respectively. Drug efficacy throughout the follow up period was much greater in patients who complied with all 3 doses.
It is unlikely that the goal of mass treatment programmes for endemic S. haematobium in villages in Africa will be realized due to poor compliance with the current dosage schedule for metrifonate of 3 doses of 7.5 mg/kg at fortnightly intervals.
Similar content being viewed by others

References
Sackett DL, Hynes B (1976) Compliance with therapeutic regimens. Johns Hopkins University Press, Baltimore
Gustafsson LL, Beermann B, Aden Abdi Y (eds) (1987) Handbook of drugs for tropical parasitic infections. Taylor and Francis, London
Jordan P (1977) Schistosomiasis-research to control. Am J Trop Med Hyg 26: 877–886
Jordan P, Webbe G (eds) (1982) Schistosomiasis: Epidemiology, treatment and control. Heinemann Medical, London
World Health Organization (1984) Epidemiological surveillance of communicable diseases in Somali Democratic Republic. National morbidity survey, 1980/1982. EM/EPID/78, EM/CD/31, WHO, Geneva
Koura M, Uptham ES, Awad AH, Ahmed MD (1981) Prevalence of Schistosoma haematobium in the Koryoole and Merca districts of the Somali Democratic Republic. Ann Trop Med Parasitol 75: 53–61
Peters PA, Warren KS, Mohamoud AAF (1976) Rapid, accurate quantification ofSchistosoma eggs via nucleopore filters. J Parasitol 62: 154–155
Daniel WW (1978) Applied nonparametric statistics. Houghton Mifflin, Boston
Davis A (1968) Comparative trials of antimonial drugs in urinary schistosomiasis. Bull WHO 38: 197–227
Greenberg RN (1984) Overview of patient compliance with medication dosing: A literature review. Clin Ther 6: 592–599
Matola YG, Malle LN (1985) Factors affecting the compliance of malaria chemosuppression with chloroquine at some maternal and child health clinics in Tanga Region Tanzania. East Afr Med J oct.; 62 (10): 721–725
MacCormack CP, Lwihula G (1983) Failure to participate in a malaria chemosupression programme, North Mara, Tanzania. J Trop Med Hyg 86: 99–107
Belcher DW, Nicholas DD, Blumenfeld (1975) Factors influencing utilization of a malaria prophylaxis programme in Ghana. Soc Sci Med 9: 241–248
Brohult J, Hedman P, Rombo L, Sirleaf V, Bengtsson E (1979) Habits of malaria chemoprophylaxis and an analysis of break-downs in a West African mining town. Ann Trop Med Parasitol 73: 327–331
Uptham S (1982) Assignment report: WHO assisted Schistosomiasis control project, World Health Organization and Ministry of Health, Mogadisho, Somali Democratic Republic July 22–August 21, 3–5
Peters PA, Mahamoud AAF, Warren KS, Ouma JH, Arap Siongok TK (1976) Field studies of a rapid accurate means of quantifying Schistosoma haematobium eggs in urine samples. Bull WHO 54: 159–162
Davis A, Bailey DR (1969) Metrifonate in urinary schistosomiasis. Bull WHO 41: 209–224
Plestina R, Davis A, Bailey DR (1972) Effect of metrifonate on blood cholinesterases in children during the treatment of schistosomiasis. Bull WHO 46: 747–759
Nagy VT, Wolf GR (1984) Cognitive predictors of compliance in chronic disease patients. Medical Care 22: 912–921
Aden Abdi Y, Gustafsson LL, Elmi SA (1987) A simplified dose schedule of metrifoante in the treatment of schistosoma haematobium infection in Somalia. Eur J Clin Pharmacol 32: 437–441
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Aden Abdi, Y., Gustafsson, L.L. Poor patient compliance reduces the efficacy of metrifonate treatment ofSchistosoma haematobium in Somalia. Eur J Clin Pharmacol 36, 161–164 (1989). https://doi.org/10.1007/BF00609189
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00609189