
Summary
Out of 3435 patients with ischaemic cerebrovascular disease 2540 cases were investigated using cerebral angiography. In 127 of them (5%) aneurysms were found, but without clinical evidence of subarachnoid haemorrhage (SAH).
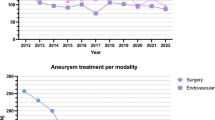
45 cases were operated upon and 82 were treated conservatively.
Five of these 82 cases (6%) suffered from SAH 3 months to 10 years (mean interval 5,6 years) after the angiographic diagnosis. Four of these 5 patients with SAH died.
Among the 45 surgical cases follow-up was uneventful in 29 (64%). The other 16 cases postoperatively showed neurological deterioration (36%), which was transient in 6 but with only minor improvement in 10. Of these 10 cases 2 died from cerebral infarction related to intra-operative temporary vascular occlusion respectively myocardial infarction. Thus surgical mortality was 4% and permanent morbidity 18%.
Causes of postoperative neurological deterioration were partly related to general arteriosclerotic changes and special fragility of the ischaemic brain, and partly to operative technique (excessive brain retraction, damage to cortical veins, occlusion of major vessels or damage to perforators, temporary artery occlusion).
Apparently in cases with ischaemic cerebrovascular diseases operative procedures, which in other cases as a rule are well tolerated, may produce harmful effects.
Therefore, in these cases, the indication for operative treatment of so far silent aneurysms should be restricted to patients who are in good general condition with longer life expectancy as far as the vascular disease is concerned, and without major neurological deficit.
Furthermore, the operative technique should be especially gentle and atraumatic.
Similar content being viewed by others

References
Asari S, Yamamoto Y (1986) New category of unruptured cerebral aneurysms. Neurol Med Chir (Tokyo) 26: 785–791
Heiskanen O (1981) Risks of bleeding from unruptured aneurysms in the cases with multiple intracranial aneurysms. J Neurosurg 55: 524–526
Heiskanen O (1986) Risk of surgery for unruptured intracranial aneurysms. J Neurosurg 65: 451–453
Jane JA, Kassell NF, Torner JC, Winn HR (1985) The natural history of aneurysms and arteriovenous malformation. J Neurosurg 62: 321–323
Kitahara S, Saito I, Segawa H, Nihei H, Okada T (1983) Operation on cerebral aneurysm complicated with cerebral infarction. In: Kodama N (ed) Proceeding of the 2nd Conference of Surgical Treatment of Stroke. Neuron, Tokyo, pp 165–168
Prezelmoski MM, Fischer M, Davidson RI, Jones HR, Marcus EM (1986) Unruptured intracranial aneurysm and transient focal cerebral ischemia: a follow-up study. Neurology 36: 584–587
Samson DS, Hodosh RM, Kemp W (1977) Surgical management of unruptured asymptomatic aneurysms. J Neurosurg 46: 731–734
Takahashi A, Ohta H, Suzuki A, Yasui N (1987) Rebleeding after clipping of aneurysm. Surg Cereb Stroke (Tokyo) 15: 116–122
Wirth FP, Laws ER Jr, Piepgras D, Scott RM (1983) Surgical treatment of incidental intracranial aneurysms. Neurosurgery 12: 507–511
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nagashima, M., Nemoto, M., Hadeishi, H. et al. Unruptured aneurysms associated with ischaemic cerebrovascular diseases. Surgical indication. Acta neurochir 124, 71–78 (1993). https://doi.org/10.1007/BF01401125
Issue Date:
DOI: https://doi.org/10.1007/BF01401125