
Summary
After improvement of technical equipment continuous ambulatory blood pressure monitoring is more and more used in the diagnosis of hypertension. New fully automatic systems permit a reliable registration and evaluation of 24-h blood pressure profiles. Typical circadian rhythmics of blood pressure, independent of a variability with different grades of activity, can be demonstrated in normotensive persons and also in patients with essential hypertension. Patients with secondary forms of hypertension show a nivellation or offset of circadian blood pressure rhythmics. A study was performed to examine the antihypertensive efficacy of the calcium antagonist Nitrendipine, theβ 1-adrenoceptor-selective blocker Metoprolol, theβ-blocker with intrinsic activity Mepindolol and the angiotensin converting enzyme inhibitor Enalapril in patients with mild to moderate hypertension over a period of 6 month. Continuous ambulatory blood pressure monitoring was performed before and after 6 month of therapy. 98 of 299 included patients broke off therapy, 47 of those because of side effects. Hydrochlorothiazide was given additionally if the antihypertensive effect of monotherapy was not sufficient after a period of 4 weeks. Morning blood pressure controls at the end of the treatment period showed normotensive values in all groups without significant differences between the groups before and at the end of the treatment period. The number of prescriptions of diuretics necessary to achieve normotension differed between the four treatment groups: Nitrendipine (n=5), Metoprolol (n=7), Mepindolol (n=14), Enalapril (n=20).
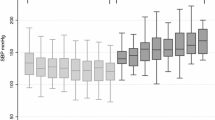
In contrast to the morning blood pressure values the continuous 24-h blood pressure monitoring demonstrated significant differences between the therapy groups. Metoprolol turned out as most effective in lowering blood pressure and in reducing the number of systolic blood pressure peaks above 180 mmHg, but on the other hand showed the highest incidence of relative hypotension (<100 mmHg systolic, <80 mmHg diastolic). Mepindolol demonstrated a significant lower efficacy. In the Nitrendipin group least of all prescriptions of diuretics were necessary and the lowest number of hypotensive systolic blood pressure values occurred. Enalapril showed the most significant reduction of diastolic values above 100 mmHg and the lowest number of diastolic values below 80 mmHg, but the highest number of prescription of diuretics was necessary in the Enalapril group. In none of the four therapy groups a neutralisation of circadian blood pressure rhythmics was demonstrable.
Zusammenfassung
Durch technische Verbesserungen der Meßgeräte findet die nichtinvasive kontinuierliche Blutdruckmessung in zunehmendem Umfang Anwendung in der Hypertoniediagnostik. Neue vollautomatische Meßgeräte erlauben eine zuverlässige Registrierung und Auswertung von 24 Stunden Blutdruckprofilen. Unabhängig von aktivitätsbedingten Blutdruckschwankungen findet sich bei normotonen Personen und auch bei Patienten mit primärer Hypertonie ein typischer circadianer Rhythmus des Blutdrucks. Patienten mit sekundären Hypertonieformen zeigen eine Abflachung oder Aufhebung des circadianen Blutdruckrhythmus. In einer Studie wurde die Wirksamkeit des Calciumantagonisten Nitrendipin, desβ 1-selektiven Blockers Metoprolol, des ISA-β-blockers Mepindolol und des ACE-Hemmers Enalapril über einen Zeitraum von 6 Monaten bei Patienten mit leichter bis mittelschwerer Hypertonie untersucht. Eine 24 h Blutdruckregistrierung erfolgte vor und nach 6-monatiger Therapie. Von 299 eingeschlossenen Patienten brachen 98 Patienten die Studie ab, davon 47 wegen unerwünschter Wirkungen. Bei nichtausreichender Wirksamkeit der Monotherapie wurde nach 4 Wochen zusätzlich Hydrochlorothiazid verordnet. Die morgendlichen Ambulanzblutdruckwerte lagen in allen Gruppen am Ende des Beobachtungszeitraums im normotonen Bereich, ohne daß signifikante Unterschiede zwischen den Gruppen vor und am Ende der Studie bestanden. Zu diesem Therapieerfolg war eine unterschiedliche Anzahl von Diuretikaverordnungen notwendig: Nitrendipin (n=5), Metoprolol (n=7), Mepindolol (n=14) und Enalapril (n=20).
Trotz der vergleichbaren morgendlichen Blutdruckwerte ergaben sich in der 24 h Blutdruck-Registrierung z.T. deutliche Unterschiede. Metoprolol zeigte den deutlichsten blutdrucksenkenden Effekt und reduzierte systolische Blutdruckspitzen über 180 mmHg am effektivsten; wies aber auch die höchste Inzidenz von relativ hypotonen Werten (<110/<80 mmHg) auf. Eine wesentlich geringere Wirkung wies Mepindolol auf. Nitrendipin benötigte die geringste Anzahl zusätzlicher Diuretikaverordnungen und wies die geringste Anzahl von hypotonen systolischen Werten auf. Enalapril wies die deutlichste Reduktion von diastolischen Werten über 100 mmHg auf, und zeigte die geringste Anzahl von diastolischen Werten unter 80 mmHg, benötigte allerdings am häufigsten ein Diuretikum. Die Blutdrucktagesrhythmik wurde in keiner der 4 Therapiegruppen aufgehoben.
Similar content being viewed by others


Literatur
Bevan AT, Honour AJ, Stott FH (1969) Direct arterial pressure recording in unrestricted man. Clin Sci 36:329–344
Devereux RB, Pickering TG, Harshfield GA, Kleinert HD, Denby L, Clark L, Pregibon D, Jason M, Sachs I, Borer JS, Laragh JH (1983) Left ventricular hypertrophy in patients with hypertension: Importance of blood pressure response to regularly recurring stress. Circulation 68:470–476
Drayer JIM, Weber MA, DeYoung JL, Wyle FA (1982) Circadian blood-pressure pattern in ambulatory hypertensive patients. Am J Med 73:493–499
Drayer JIM, Weber MA (1985) Definition of normalcy in whole-day ambulatory blood-pressure monitoring. Clin Exp Hypertens A7:195–204
Drayer JIM (1985) The dilemma of mild hypertension. Noninvasive evaluations of hypertensive patients. Chest 3 (Suppl):183S-186S
Fritzgerald DJ, O'Malley K, O'Brien ET (1984) Reproducibility of ambulatory blood-pressure recordings. In: Weber MA, Drayer JIM (eds) Ambulatory blood-pressure monitoring. Steinkopff, Darmstadt, pp 71–74
Harshfield GA, Pickering TG, Phil D, Kleinert HD, Blank S, Laragh JH (1982) Situational variations of blood pressure in ambulatory hypertensive patients. Psychosomatic Med 44:237–245
Harshfield GA, Pickering TG, Blank S, Lindahl C, Stroud L, Laragh JH (1984) Ambulatory blood-pressure monitoring: recorders, applications and analyses. In: Weber MA, Drayer JIM (eds) Ambulatory blood-pressure monitoring. Steinkopff, Darmstadt, pp 1–8
Jacot des Combes BJ, Porchet M, Waeber B, Brunner HR (1984) Ambulatory blood pressure recordings. Reproducibility and Unpredictability. Hypertension 6:110–114
Jason M, Devereux RB, Borer JS, Pickering T, Fisher J, Harshfield G, Berkowitz A, Laragh J (1983) 24-h arterial pressure measurement: Improved prediction of left ventricular dysfunction in essential hypertension. Am J Cardiol 1:599
Kennedy HL, Horan MJ, Sprague MK, Padgett NE, Shriver KK (1983) Ambulatory blood pressure in healthy normotensive males. Am Heart J 106:717–722
Magometschnigg D (1988) Vom Nutzen der indirekten 24-Stunden-Blutdruckmessung und der Blutdruckselbstkontrolle für die Diagnostik der arteriellen Hypertonie. WMW 138:40–43
Mann S, Millar-Craig MW, Rafter B (1985) Superiority of 24-hour measurements of blood-pressure over clinic values in determining prognosis in hypertension. Clin Exp Hypertens 7:279–282
Meyer-Sabellek W, Sehested J, Schulte K-L, Gotzen R (1984) Clinical significance of cardiovascular rhythms and applicability of invasive, and non-invasive methods for 24-h blood-pressure monitoring. In: Kimmich HP, Klewe H-J (eds) Biotelemetry VIII. Drönig, Braunschweig, pp 183–186
Millar-Craig MW, Bishop CN,Raftery EB (1978) Circadian variation of blood-pressure. Lancet I:795
Nomura A, Yasuda H, Kato K, Shimono H, Murakami T, Minami M, Takechi S (1985) Direct blood-pressure monitoring in patients with pheochromocytoma. Jpn H J 26:845–849
Perloff D, Sokolow M, Cowan R (1983) The prognostic value of ambulatory blood-pressure. J Am Med Ass 249:2793
Pessina AC, Palatini P, Sperti G, Cordone L, Ventura F, Dal Palu PC (1984) Adaptation ton non-invasive continuous blood-pressure monitoring. In: Weber MA, Drayer JIM (eds) Ambulatory blood pressure monitoring. Steinkopff, Darmstadt, pp 57–64
Pickering TG, Harshfield GA, Laragh JH (1980) Use of ambulatory blood-pressure monitoring in the evaluation of patients with borderline hypertension. Am J Cardiol 45:446–448
Pickering TG, Harshfield GA, Kleinert HD, Blank S, Laragh JH (1982) Blood-pressure during normal daily activities, sleep, and exercise. J Am Med Ass 247:992–996
Pickering TG, Harshfield GA, Devereux RB, Laragh JH (1985) What is the role of ambulatory blood pressure monitoring in the management of hypertensive patients? Hypertension 7:171–177
Richardson DW, Honour AJ, Tenton GW, Pickering GW (1964) Variation in arterial pressure throughout the day and night. Clin Sci 26:445–460
Rowlands DB, Ireland MA, Glover DR, McLeay RAB, Stallard TJ, Littler WA (1981) The relationship between ambulatory blood pressure and echocardiographically assessed left ventricular hypertrophy. Clin Sci 61 (Suppl):101S-103S
Sleight P (1985) Differences between casual and 24-h blood-pressure. J Hypertension 3 (Suppl 2):19–22
Sokolow M, Wedegar D, Kain HK, Hinman AT (1966) Relationship between level of blood-pressure measured casually and by portable recorders and severity of complications in essential hypertension. Circulation 34:279
Vetter W, Vetter H (1987) 24-Stunden-Blutdruckmessung: Einsatz in Klinik und Praxis. Schweiz. Rundschau Med 76:441–472
Weber MA, Drayer JIM (1984) The circadian blood-pressure pattern in ambulatory normal subjects. Am J Cardiol 54:115–119
Wikstrand J, Warnold I, Olsson G, Tuomilehto J, Elmfeldt D, Berglund G (1988) Primary prevention with metoprolol in patients with hypertension. Mortality results from the MAPHY-Study. JAMA 259:1976–1982
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Schrader, J., Schoel, G., Buhr-Schinner, H. et al. Ambulante kontinuierliche 24 h Blutdruckregistrierung in der Diagnostik und Therapie der arteriellen Hypertonie und die Beeinflussung durch die Antihypertensiva Enalapril, Metoprolol, Mepindolol und Nitrendipin. Klin Wochenschr 66, 928–939 (1988). https://doi.org/10.1007/BF01728957
Issue Date:
DOI: https://doi.org/10.1007/BF01728957